Kingu Kurimuzon
Well-known member
- Joined
- Aug 27, 2013
- Messages
- 20,940
- MBTI Type
- I
- Enneagram
- 9w8
- Instinctual Variant
- sp/sx
Shit
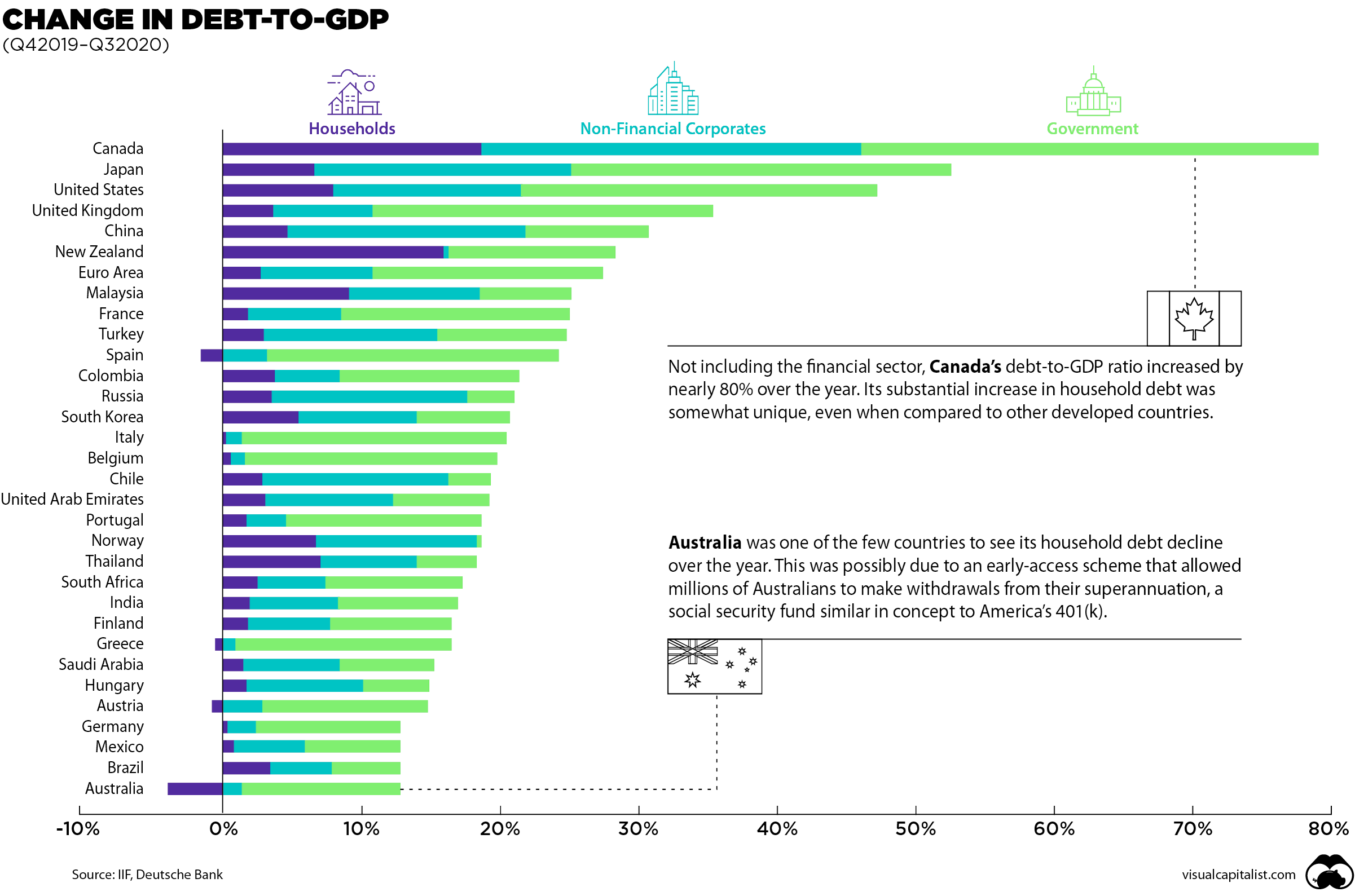
Or how the world seems to be going broke.
Bankers will profit over this, as usual.
Basically, capitalism today seems to program profit for bankers regardless of what happens.
If the apocalypse came by, the bankers would probably still profit from it.
If suffering increases due to this, it doesn't matter [to them].
Wow. I have heard concern expressed about Canada, and it looks out of control on this chart.Or how the world seems to be going broke.
I find it telling that people talking about the climbing suicide rates seem to not grasp that the reason for suicides was frequently the same reason BEFORE Covid.
Poverty, lack of health care access, lack of health care affordability, lack of child care, lack of jobs, lack of food access - the total bootstraps brainwashing in the US. A government so derelict in its concern for its people then add the last 4 years of chaotic stupidity plus the absence of a comprehensive federal response to the pandemic - it's fucking obvious that it's MUCH more than just the lockdown.
The UK paper also cites these things, Psychology Today does not.
Link didn't work for me. Is it because. Coughing instinctively makes people back away, whereas transmission via talking sneaks up on people unawares (because it's easy to still keep forgetting that we're sticking our faces into a pool of someone else's exhale)? Or is talk exhale actually somehow more loaded with contamination than cough exhale?
^I remember reading something similar about single layer, polyester/nylon masks and/or gators; instead of blocking the particles, it breaks them up into smaller pieces which linger longer in the air than if a person weren't wearing any face covering at all. But maybe it wasn't accurate, because I can't find anything about it now.
I think it was more about those pieces of thin fabric that ties behind the head but hangs loose. They're not gaters, they're like face scarves. But I see more and more places banning anything that doesn't fit the face snugly which is sensible in terms of particle blocking.
Coming from both the left and right, and around the world, we have devoted our careers to protecting people. Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
Fortunately, our understanding of the virus is growing. We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.
As immunity builds in the population, the risk of infection to all – including the vulnerable – falls. We know that all populations will eventually reach herd immunity – i.e. the point at which the rate of new infections is stable – and that this can be assisted by (but is not dependent upon) a vaccine. Our goal should therefore be to minimize mortality and social harm until we reach herd immunity.
The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
...
Those who are not vulnerable should immediately be allowed to resume life as normal.
Results of the study: COVID-19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
Conclusions drawn from the study and clinical implications: The specific and significant COVID-19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.